
A single male 21 year-old subject (mass 60 kg, height 1.68 m) was selected. Anthropometric measurements (lower-limb lengths, knee and ankle widths) were recorded, and 25 mm retroreflective markers attached to the following sites: spinous process of the second sacral vertebra (S2, between the sacral dimples), both anterior superior iliac spines (L&RASIS), lateral malleoli, and heads of both second metatarsals. The knee joint center of each leg was then identified by making a series of marks on the lateral femoral condyle, until one was found which showed least movement when the knee was flexed. When correctly located, the anterior edge of the knee marker was noted (from experience) to bisect the antero-posterior dimension of the knee joint.
The subject was then orientated such that the operator could see a sagittal plane view of the subject in a mirror situated some 3 m distant (fig. 2). On identifying the location of the greater trochanter (hip joint center, HJC) with the index finger of one hand, the thigh wand was then attached such that the HJC, knee marker and thigh wand marker were co-linear. It should be noted that optimal alignment of the thigh wand is difficult and many techniques (e.g. the knee alignment device manufactured by Motion Lab Systems, Baton Rouge, LA, USA) have been described for improving consistency and accuracy. The method described here was found most convenient by the present author, but no technique is completely foolproof (Baker et al, 1999).
Fig. 2: Attaching the thigh wands with the aid of a mirror. The operator adjusts the wand until it is co-linear with the HJC (greater trochanter, indicated by the assistant) and knee marker.
The shank (tibial) wands were finally attached by lining up the foot in the sagittal plane and using the mirror to ensure co-linearity with the knee and lateral malleolus markers.
Following a static trial (in which calcaneal markers were also attached), the subject was requested to walk repeatedly along a 10 m walkway, in which two force platforms (Advanced Medical Technologies, Boston MA, USA) were mounted. A six-camera infra-red video-based motion analysis system (Vicon 370, version 2.6, Vicon Medical Systems, Oxford, UK) was then used to track the markers and reconstruct the motion in three dimensional space.
Several preliminary trials were recorded and analyzed using the MHH model in order to confirm correct placement of the markers. In particular, the knee frontal plane angle was examined for varus-valgus artefacts (see below) and the knee sagittal plane angle was checked for flexion or extension offsets (see below). Once these were satisfactory, several trials of natural gait were recorded.
In order to investigate the effect of erroneous marker placement, the following interventions were made and repeat gait trials recorded:
1) The right knee marker was moved one diameter first anterior, then posterior (the nominal position having been marked during the original attachment);
2) The right thigh wand was angulated first anterior, then posterior by a few degrees. The precise amount was not quantified, but corresponded to the range commonly encountered during CGA (about ± 50 mm).
3) The sacral marker was reattached one spinous process above and below S2.
4) The right ASIS marker was reattached one diameter medial and lateral.
The marker trajectory data so collected was analyzed by the MHH model, using the Plug-in-Gait module of the Vicon Workstation software. Gait curves were then plotted using Vicon Polygon.
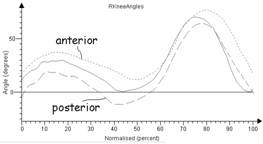
Fig. 3: Effect of errors in knee joint center marker on knee flexion angle.
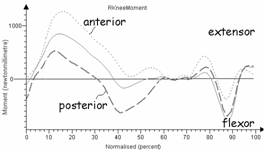
Fig. 4: Effect of errors in knee joint center marker on knee joint moment.
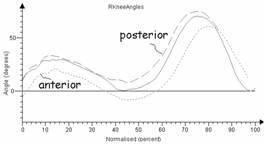
Fig. 5: Effect of errors in thigh wand angulation on knee flexion angle.
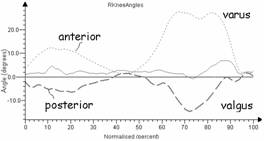
Fig. 6: Effect of errors in thigh wand marker on frontal plane knee angle (varus-valgus artefact).
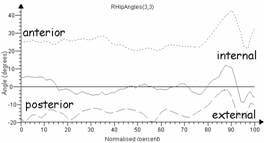
Fig. 7: Effect of errors in thigh wand angulation on hip rotation.
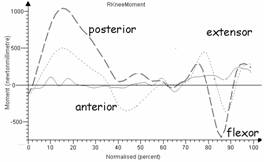
Fig. 8: Effect of errors in thigh wand angulation on knee extensor moment.
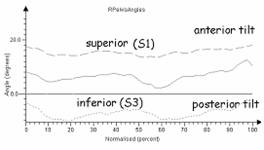
Fig. 9: Effect of errors in sacral marker placement on pelvic tilt.
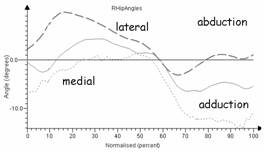
Fig. 10: Effect of errors in right ASIS marker on right hip abduction-adduction.
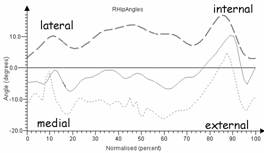
Fig. 11: Effect of errors in right ASIS marker on right hip rotation.
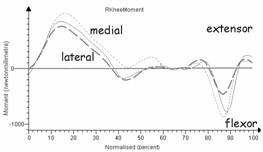
Fig. 12: Effect of errors in right ASIS marker on right knee extensor moment.
As might be expected, �errors� in placement of the marker on the knee joint center introduced a flexion or extension offset according to whether the marker was anterior or posterior to its correct position (fig. 5). In the latter position, the result was to mimic a genu recurvatum. Peak stance and swing phase flexion were also affected, as was the angle of the knee at initial contact, all of which are important clinical parameters. In addition, the peak knee moment became more extensor or flexor, respectively, by around 250 Nmm/kg (some 30% of nominal) during stance.
Angulation of the thigh wand anteriorly or posteriorly, perhaps less obviously, also induced extension or flexion errors. The reason for this is that the thigh wand is used to determine the knee joint axis � if it is deflected anteriorly, the axis will rotate medially (internally). Since the knee marker remains fixed, this has the effect of moving the knee centre posteriorly, thereby introducing an extension offset.
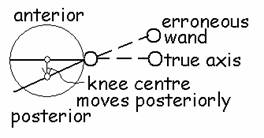
Fig. 15: Effect of an angulated thigh wand on knee joint center.
The thigh wand also has a marked effect on the knee angle in the frontal plane (fig. 6). In effect, suboptimal alignment causes �crosstalk� from the sagittal plane to appear in the frontal plane curve. This phenomenon is well known as the �varus-valgus� artefact, and can be used by the astute gait analyser as a quality control aid, since (at least in subjects with intact collateral ligaments) there should normally be almost no frontal plane motion at the knee (Baker et al, 1991). The two artifacts are roughly symmetrical, but it is interesting to note that the varus artefact is usually more prominent and often (as here) shows a �double hump� in swing phase.
Knee varus-valgus angle is not usually an important clinical parameter. However, it is clear that errors in thigh wand angulation have consequences on another rather more important clinical variable: hip rotation (fig. 7). In essence, the thigh wand sets the frontal plane of the thigh, and, if it is angulated anteriorly or posteriorly, it will introduce an internal or external rotation to the hip kinematics.
Also of potential clinical impact are the effects on knee moment. Due to the phenomenon discussed above, thigh wand angulation introduces an antero-posterior shift in the knee joint center, which consequently affects the moment calculated about that center.
Errors in the sacral marker height were predictable, in that an superior displacement introduced an anterior tilt and vice versa. The magnitude of the error ( ± 100%) is worth noting, however, since it is sometimes not an easy task to locate vertebrae in obese or uncooperative subjects.
Finally, error in placement of the ASIS marker was also significant. To understand why, it is necessary to know how the HJC is determined in the MMH model. Movement of the marker medially or laterally will relocate the HJC in the corresponding direction, causing hip abduction-adduction to be affected (fig 10) but also introducing large errors in the hip rotation profile (fig. 11), and, to a lesser extent, the knee moment (fig. 12). Once again, to understand why necessitates insight into the way in which the HJC is estimated by the MHH model.
In summary, results derived from the MHH model are exquisitely sensitive to marker placement. In view of the clinical implications, the routine clinical use of this model must surely be called into question, and may account for much of the known inter-laboratory variability. The model�s weakness is its reliance upon bony landmarks. Models based on marker clusters may therefore offer advantages in this regard.
Baker R, et al (1999) A New Approach to determine the Hip Rotation Profile from Clinical Gait Analysis Data, Human Movement Science 18(5): 655-667.
Davis, et al (1991) A gait data collection and reduction technique. Human Movement Sciences 10, 575-587.